Φάρμακα για τον COVID-19:Μια βαθιά κατάδυση στη Βιοχημεία και τους Μηχανισμούς
Βασικές έννοιες
Σε αυτό το άρθρο, θα διερευνήσετε τη βιοχημική βάση που βρίσκεται κάτω από ορισμένα από τα πιο συχνά χρησιμοποιούμενα φάρμακα για τον COVID-19. Θα μάθετε για τους μηχανισμούς δράσης, τις φαρμακοκινητικές αρχές και τη χρησιμότητα τους στην καταπολέμηση του τρομερού ιού SARS-CoV-2. Θα εξοικειωθείτε επίσης με τους φαρμακευτικούς στόχους, το αυξανόμενο πρόβλημα της αντιϊκής αντοχής και τις συμπληρωματικές και συμπληρωματικές επιλογές θεραπείας για τον COVID-19.
Αυτό είναι το πέμπτο άρθρο μιας ειδικής μίνι σειράς ChemTalk σχετικά με τις τομές μεταξύ της χημείας και της δημόσιας υγείας, χρησιμοποιώντας το COVID-19 ως μελέτη περίπτωσης. Σε αυτήν τη σειρά, μπορείτε να αναμένετε να μάθετε για τις διαδικασίες ανακάλυψης και ανάπτυξης φαρμάκων, τον κεντρικό ρόλο της χημείας στη διάγνωση και την πρόληψη ασθενειών και τις καριέρες που βρίσκονται στην πρώτη γραμμή της χημείας και της δημόσιας υγείας.
Άλλα άρθρα σε αυτήν τη μίνι σειρά
Η Χημεία Πίσω από τους Κορωνοϊούς
Η Διαδικασία Ανακάλυψης Φαρμάκων
Η Διαδικασία Ανάπτυξης Φαρμάκων
Καριέρες Χημείας στον Τομέα Δημόσιας Υγείας
The Disease Detective Work of Lab Diagnostics
Επιστημονικές Στρατηγικές για την Πρόληψη Νοσημάτων
Χημεία, Δημόσια Υγεία και Εσείς
Πώς επηρέασε ο COVID-19 τη διαδικασία ανάπτυξης φαρμάκων;
Μέχρι τώρα, έχουμε περιηγηθεί στα ρυθμισμένα βήματα της φαρμακευτικής διαδικασίας και στους πολλούς επαγγελματίες βιοϊατρικούς που δημιουργούν φάρμακα. Αυτό αντιπροσωπεύει την «κανονική» εικόνα του πώς φαίνεται η ανάπτυξη φαρμάκων. Αλλά κατά τη διάρκεια μιας κρίσης υγείας όπως μια πανδημία, καθώς οι επιδημιολογικές συνθήκες αλλάζουν γρήγορα, αυτή η εικόνα μπορεί επίσης να αλλάξει γρήγορα.
Η ανταπόκριση της δημόσιας υγείας στον COVID-19 έκανε ταχυδακτυλουργικά πολλά κινούμενα μέρη. Κάθε φορά που μια συγκεκριμένη πόλη δαμάζει ένα τοπικό ξέσπασμα, μια άλλη εμφανιζόταν αλλού, φαινομενικά χωρίς να παρακάμψει το ρυθμό. Ολόκληρες βιομηχανίες υπέστησαν σοβαρές οικονομικές επιπτώσεις, και ορισμένες εξακολουθούν να ανακάμπτουν στις μέρες μας. Οι συνέπειες της μακροχρόνιας κοινωνικής απομόνωσης άλλαξαν τον τρόπο με τον οποίο αλληλεπιδρούμε μεταξύ μας και επηρέασαν την ψυχική υγεία ορισμένων ανθρώπων. Όλο αυτό το διάστημα, οι επαγγελματίες υγείας έπρεπε να διαχειρίζονται κύματα ασθενών κάτω από πιεσμένη ιατρική υποδομή.
Ένα άλλο στοιχείο που έπρεπε να αλλάξει κατά την έναρξη της πανδημίας ήταν η διαδικασία ανάπτυξης φαρμάκων. Αυτό που είναι συνήθως μια πολύ οργανωμένη, τυποποιημένη επιχείρηση προσπαθούσε ξαφνικά να συμβαδίσει με το εξελισσόμενο κοινωνικό, οικονομικό και πολιτικό έδαφος της πανδημίας. Οι βιοϊατρικοί ερευνητές κινητοποιήθηκαν σε μια συντονισμένη προσπάθεια για τη δημιουργία και τη δοκιμή θεραπειών για τον COVID-19 και τελικά πέτυχαν με την παραγωγή νέων φαρμάκων και εμβολίων που εντοπίζουν τον SARS-CoV-2, τον ένοχο πίσω από τον COVID-19.
Σε αυτό το άρθρο, θα επικεντρωθούμε στον τρόπο με τον οποίο λειτουργούν μερικά αντιπροσωπευτικά φάρμακα για τον COVID-19 και πώς ταιριάζουν στην γενική αντιμετώπιση της πανδημίας. Προς το παρόν, ας κάνουμε ένα βήμα πίσω από αυτή τη μεγάλη οπτική γωνία και ας μεγεθύνουμε τις λεπτομέρειες μικρότερης κλίμακας για το πώς αυτά τα φάρμακα συνέβαλαν στην αποτροπή μιας από τις χειρότερες κρίσεις υγείας της εποχής μας.
Γιατί τα αντιιικά φάρμακα χρησιμοποιούνται ως θεραπείες για τον COVID-19;
Δεδομένου ότι στοχεύουν τον ιό SARS-CoV-2, τα φάρμακα για τον COVID-19 είναι ένας τύπος αντιικού φαρμάκου . Σε σύγκριση με άλλα παθογόνα, οι ιοί μπορεί να είναι ιδιαίτερα δύσκολο να αντιμετωπιστούν, για λόγους που θα συζητήσουμε εκτενέστερα σύντομα. Δεν μπορούμε να «θεραπεύσουμε» ή να εξαλείψουμε ιογενείς ασθένειες με την αυστηρή έννοια, αλλά μπορούμε να διαχειριστούμε τα συμπτώματά τους όσο ο ιός τρέχει. Τα αντιιικά φάρμακα αποσκοπούν συχνά στη μείωση των σωματικών συμπτωμάτων και στην πρόληψη της εξάπλωσης της νόσου σε άλλους όσο ο ασθενής αναρρώνει.
Τα αντιιικά φάρμακα έρχονται σε πλήρη αντίθεση με τα αντιβιοτικά , τα οποία χρησιμοποιούνται για τη θεραπεία λοιμώξεων όπου το παθογόνο είναι ένα βακτήριο. Τα αντιβιοτικά έχουν τη θέση τους, αλλά ποτέ δεν ήταν μια ρεαλιστική επιλογή θεραπείας για τον COVID-19, επειδή το COVID-19 προκαλείται από έναν ιό και όχι από ένα βακτήριο. Οι τεχνικές εξόντωσης βακτηρίων που χρησιμοποιεί ένα αντιβιοτικό δεν κάνουν τίποτα για να νικήσουν έναν ιό — θα ήταν σαν να προσπαθείς να φας σούπα με ένα πιρούνι.
Αντίθετα, πρέπει να μαγειρέψουμε ένα φάρμακο που αξίζει να κερδίσουμε ενάντια σε έναν ιό. Όταν αναπτύσσουν ένα αντιιικό φάρμακο, οι ερευνητές αξιολογούν πρώτα πώς λειτουργεί ο συγκεκριμένος ιός:πώς εισέρχεται στο σώμα, πώς μολύνει τα υγιή κύτταρα, πώς εξαπλώνεται μεταξύ των ανθρώπων και πολλά άλλα. Κατανοώντας τον μηχανισμό του ιού, οι ερευνητές μπορούν στη συνέχεια να προσδιορίσουν τον μηχανισμό του φαρμάκου. Το φάρμακο πρέπει να λειτουργεί με τρόπο που διακόπτει ή ελαχιστοποιεί την κανονική λειτουργία του ιού.
Αυτή η στρατηγική προσέγγιση αντικατοπτρίζει τα πρώτα στάδια της ευρύτερης ανακάλυψης ναρκωτικών διαδικασία, μέσω της οποίας οι βιοϊατρικοί επιστήμονες κάνουν τα πρώτα βήματα στο σχεδιασμό ενός φαρμάκου. Οι κορωνοϊοί όπως ο SARS-CoV-2 κλέβουν τον μηχανισμό μοριακής βιολογίας των υγιών κυττάρων για να αναπαράγουν το δικό τους γενετικό υλικό. Γνωρίζοντας αυτό, οι ερευνητές εστίασαν τις προσπάθειές τους στο σχεδιασμό ενός φαρμάκου που θα παρεμπόδιζε την ικανότητα του ιού να εισέλθει ή να χρησιμοποιήσει τα κύτταρα ξενιστές. Εάν αυτές οι διεργασίες μπορούσαν να συγκρατηθούν, το ίδιο θα μπορούσε να γίνει ο SARS-CoV-2 και η πανδημία συνολικά. Έτσι, αυτό έθεσε το επόμενο κρίσιμο ερώτημα:Πώς μπορούμε να φτιάξουμε ένα αντιικό φάρμακο που εμποδίζει τις τυπικές τακτικές του SARS-CoV-2;
Ίσως να θυμάστε ότι συζητήσαμε τις συνήθεις τεχνικές ανακάλυψης φαρμάκων, καθώς και τον τρόπο λειτουργίας δύο παραδειγμάτων φαρμάκων, νωρίτερα σε αυτήν τη μίνι σειρά άρθρων. Σε αυτήν την ενότητα, θα επανεξετάσουμε τη δημιουργία ενός από αυτά τα φάρμακα για τον COVID-19, καθώς και το προηγούμενο, από τη σκοπιά της χημείας. Αυτό το καθήκον καθοδήγησε την πορεία της προσέγγισης των επιστημόνων για την επίλυση της πανδημίας. Με τιμόνι από βιοϊατρικούς ερευνητές, τα φαρμακευτικά εργαστήρια έγιναν σύντομα κέντρο ελέγχου της αποστολής. Αλλά τι ακριβώς συνέβη μέσα σε αυτά τα εργαστήρια για να υλοποιηθούν τα φάρμακα για τον COVID-19;
Κατακτώντας τα φάρμακα για τον COVID-19
Είναι αρχές του 2020 και η αναζήτηση για ένα φάρμακο για τον COVID-19 βρίσκεται σε εξέλιξη καθώς ο SARS-CoV-2 προκαλεί ενεργά καταστροφή σε όλο τον κόσμο. Ερευνητικές ομάδες σε όλο τον κόσμο αναπτύσσουν ανεξάρτητα και συνεργατικά υποψήφια φάρμακα που ελπίζουμε ότι θα νικήσουν αυτό το θηρίο ζωύφιου. Τι συνεπάγεται όμως αυτή η διαδικασία; Και τι σημαίνει για τους ασθενείς που περιμένουν με αγωνία την ανακούφιση;
Μόλις ο COVID-19 είχε κλιμακωθεί σε πανδημία, οι επιστήμονες γνώριζαν ότι δεν υπήρχε χρόνος για χάσιμο. Οι ασθενείς, οι επαγγελματίες υγείας, οι επιχειρήσεις, οι κυβερνήσεις και το ευρύ κοινό βασίζονταν σε αυτούς για να αναπτύξουν μια ασφαλή, αποτελεσματική θεραπεία που θα μπορούσε να διανεμηθεί εύκολα. Υπό το φως της ταχείας εξάπλωσης της νόσου και των προκλήσεων της εφοδιαστικής αλυσίδας που συμβαίνουν στο παρασκήνιο, αυτά τα χαρακτηριστικά του φαρμάκου ήταν ζωτικής σημασίας. Μεταξύ των πιο συνηθισμένων φαρμάκων για τον COVID-19 σήμερα — ένα που πέτυχε με επιτυχία αυτά τα κριτήρια — είναι ένα αντιικό φάρμακο που ονομάζεται nirmatrelvir/ritonavir . Ίσως γνωρίζετε αυτό το φάρμακο καλύτερα με το εμπορικό του όνομα, Paxlovid. Ας μιλήσουμε εν συντομία για το πώς οι βιοϊατρικοί επιστήμονες δημιούργησαν φάρμακα για τον COVID-19 όπως αυτό, ακόμη και στην τύχη του χρόνου.
Όλοι αγαπούν μια ιστορία επιστροφής:Η παραγωγή φαρμάκων για τον COVID-19
Βάλτε τον εαυτό σας στη θέση ενός φαρμακευτικού ερευνητή που μόλις εντόπισε τα χαρακτηριστικά του ιδανικού φαρμάκου για τον COVID-19. Ακολουθεί το πιο σημαντικό μέρος, και ίσως το μεγαλύτερο εμπόδιο που θα αντιμετωπίσετε:Πώς θα τα καταφέρετε πραγματικά; Πώς μπορείτε να χειριστείτε τη χημεία μερικών πρόδρομων ουσιών για να αποδώσετε το μόριο που θέλετε; Έχοντας ήδη καθορίσει τις ιδιότητες που θα κάνουν το φάρμακό μας να λειτουργήσει, τώρα πρέπει να εξετάσουμε προσεκτικά τη διαδικασία παρασκευής του ίδιου του φαρμάκου. Θα το αξιολογήσουμε στο πλαίσιο τριών ενώσεων που χρησιμοποιούνται ως φάρμακα για τον COVID-19.
Nirmatrelvir/Ritonavir και Lufotrelvir
Υπάρχουν μερικά πράγματα που χρειαζόμαστε από μια δυνατή συνθετική διαδρομή. Η καλύτερη προσέγγιση σύνθεσης θα χρησιμοποιούσε λίγα αρχικά υλικά για να ελαχιστοποιήσει το οικονομικό κόστος της ανάπτυξης φαρμάκων. Θα χρησιμοποιούσε επίσης γρήγορες αντιδράσεις, επιταχύνοντας τη διαδικασία παραγωγής φαρμάκου, ώστε το φάρμακο να μπορεί να φτάσει στους ασθενείς γρηγορότερα. (Αυτό το σημείο ήταν ιδιαίτερα πολύτιμο κατά την παρασκευή φαρμάκων για τον COVID-19 κατά τη διάρκεια των βαρύτερων κυμάτων της πανδημίας!) Θέλουμε επίσης η στρατηγική μας να έχει ως αποτέλεσμα όσο το δυνατόν λιγότερα παραπροϊόντα, ώστε να μεγιστοποιηθεί η καθαρότητα του φαρμάκου και να αποφευχθεί η περιττή σπατάλη. Η χημική σύνθεση χαμηλής προσπάθειας και υψηλής απόδοσης βελτιώνει τα αποτελέσματα του κατασκευαστή φαρμακευτικών προϊόντων και τελικά μεταφράζεται σε πιο αποτελεσματική παραγωγή φαρμάκων.
Ενώ οι ερευνητές επαναχρησιμοποίησαν το ritonavir (το οποίο υπήρχε ήδη ως φάρμακο για τον HIV) για τη θεραπεία του COVID-19, το nirmatrelvir συντέθηκε από την αρχή. Είναι απόγονος ενός άλλου μορίου, του lufotrelvir , το οποίο έχει πραγματικά μελετηθεί και σε κλινικές δοκιμές COVID-19. Όπως θα δούμε σύντομα, η διάκριση μεταξύ του nirmatrelvir και του lufotrelvir έγκειται λιγότερο στον τρόπο λειτουργίας τους (και τα δύο είναι αναστολείς πρωτεάσης) και περισσότερο στον τρόπο με τον οποίο χορηγούνται στο σώμα του ασθενούς.
Κατακτάς μια πανδημία; Cya-Κανένα πρόβλημα!
Στην ανάπτυξη φαρμάκων, υπάρχουν συχνά πολλά μέσα για την επίτευξη του ίδιου τελικού προϊόντος. Αυτό που έχει μεγαλύτερη σημασία είναι το μόριο με το οποίο καταλήγετε, εάν έχει τις σωστές λειτουργικές ομάδες στα σωστά σημεία και εάν επιτυγχάνει τους θεραπευτικούς του στόχους. Η σύνθεση μιας νέας ένωσης από μια προϋπάρχουσα τείνει να είναι μια εύκολη επιλογή επειδή το μοριακό πλαίσιο της επιθυμητής ένωσης υπάρχει ήδη στο αρχικό υλικό. Για να φτιάξουν το nirmatrelvir, οι επιστήμονες ξεκίνησαν με τον σκελετό μιας τριπεπτιδικής αλυσίδας.
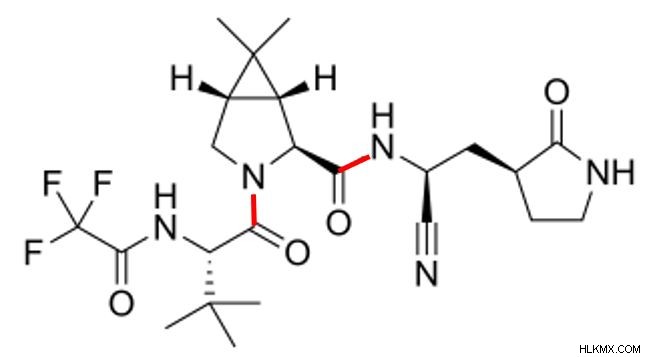 Η χημική δομή του Nirmatrelvir. Δώστε ιδιαίτερη προσοχή στους δύο πεπτιδικούς δεσμούς του και στην κυανό λειτουργική του ομάδα.
Η χημική δομή του Nirmatrelvir. Δώστε ιδιαίτερη προσοχή στους δύο πεπτιδικούς δεσμούς του και στην κυανό λειτουργική του ομάδα. Υπάρχουν δύο σημαντικά σημεία που πρέπει να κατανοήσουμε σχετικά με αυτή τη μοριακή μορφή. Πρώτον, αν κοιτάξουμε προσεκτικά το nirmatrelvir, μπορούμε να δούμε δύο πεπτιδικούς δεσμούς μέσα στη δομή του (που επισημαίνονται με κόκκινο παραπάνω). Αυτή είναι μια ένδειξη ότι το nirmatrelvir αποτελείται από τρία πεπτίδια ενωμένα μεταξύ τους. Σε αυτή την περίπτωση, τα τρία εν λόγω πεπτίδια δεν υπάρχουν στη φύση. οι συνθετικοί χημικοί τα έχουν τροποποιήσει. Η σύνθεση του nirmatrelvir περιλαμβάνει την εκτέλεση μιας σειράς αντιδράσεων συμπύκνωσης για να σχηματιστούν οι πεπτιδικοί δεσμοί και να ενωθούν τα τρία πεπτίδια σε ένα μόνο μόριο.
Δεδομένου ότι τα πεπτίδια που περιλαμβάνουν το nirmatrelvir δεν υπάρχουν στη φύση, το nirmatrelvir είναι ένα πεπτιδομιμητικό μόριο. Τα πεπτιδομιμητικά μοιάζουν με πεπτίδια και μιμούνται τις λειτουργίες τους, αλλά επειδή είναι συνθετικά, συχνά παρακάμπτουν τα προβλήματα που παρουσιάζουν οι φυσικές πρωτεΐνες. Ανάλογα με το εν λόγω πεπτιδομιμητικό μόριο, μπορεί να εμφανίζει καλύτερη σταθερότητα, επιλεκτικότητα ή ισχύ από τα πραγματικά πεπτίδια. Όλοι αυτοί οι παράγοντες επηρεάζουν τα αποτελέσματα του φαρμάκου, όπως το πόσο διαρκεί στον οργανισμό και πόσο καλά στοχεύει το παθογόνο που μας ενδιαφέρει. Έτσι, το μεγαλύτερο πλεονέκτημα ενός πεπτιδομιμητικού φαρμάκου είναι ότι επιτρέπει στους ερευνητές να προσαρμόσουν, μέσω χημικής σύνθεσης, τη συμπεριφορά του ώστε να ταιριάζει στις ανάγκες ενός συγκεκριμένου σχεδίου θεραπείας. Κατά την καταπολέμηση ενός ιού που κινείται συνεχώς και είναι δύσκολο να εντοπιστεί, ένα εξατομικευμένο πεπτιδομιμητικό φάρμακο είναι σαν ένα βλήμα που αναζητά θερμότητα:ισχυρά ακριβές και στερεωμένο στον στόχο του.
Δεύτερον, βλέπουμε ότι το nirmatrelvir είναι ο περήφανος ιδιοκτήτης ενός τριπλού δεσμού άνθρακα-αζώτου, ένα χαρακτηριστικό που δεν υπάρχει στον πρόγονό του lufotrelvir. Η υψηλής ενέργειας, σχετικά ασταθής ομάδα κυανό είναι κρίσιμης σημασίας για τη λειτουργία του nirmatrelvir ως φάρμακο για τον COVID-19. Ονομάζεται «ηλεκτρόφιλη κεφαλή», είναι η οντότητα που στοχεύει τις κυριότερες πρωτεάσες (Mpro ) που οδηγούν την αναπαραγωγή του SARS-CoV-2. Όταν η κυανό ομάδα του nirmatrelvir έρχεται σε άμεση επαφή με το υπόλειμμα κυστεΐνης του Mpro, αναστέλλει την ικανότητα του Mpro να παράγει πρωτεΐνες που χρησιμοποιεί ο ιός για την αναπαραγωγή. Μεταξύ των μελών της οικογένειας των κοροναϊών, τα μόρια Mpro διατηρούνται σε μεγάλο βαθμό. Αυτό συμβαίνει επειδή έχουν θεμελιώδη ρόλο στον κύκλο ζωής των ιών, αλλά αυτή η διατήρηση εξοπλίζει επίσης το nirmatrelvir για την καταπολέμηση πολλών διαφορετικών παραλλαγών του κορωνοϊού. Είναι βαθύ ότι ένα τόσο μικροσκοπικό ζεύγος ατόμων έχει έντονο αποτέλεσμα στη λειτουργία του φαρμάκου και, φυσικά, στην πρόγνωση του ασθενούς.
The Buddy System:Ο ρόλος του Ritonavir στην καταπολέμηση του COVID-19
Ωστόσο, το nirmatrelvir δεν μπορεί να τα κάνει όλα αυτά μόνο του. Λειτουργεί πολύ καλύτερα με την υποστήριξη μιας άλλης ένωσης, της ριτοναβίρης, καθώς πραγματοποιούν αυτή την απαιτητική προσπάθεια μαζί. Αφού ο ασθενής καταναλώσει μια δόση νιρματρελβίρης, αυτό (όπως κάθε χάπι) υπόκειται στη μεταβολική οργή του πεπτικού συστήματος του σώματος. (Περισσότερα για αυτό αργότερα!) Προς το παρόν, θα πρέπει να καταλάβετε ότι οι πεπτικές δυνάμεις του σώματος διασπούν τα χάπια με την πάροδο του χρόνου. Όσο πιο γρήγορα διασπάται το χάπι, τόσο πιο σύντομη θα διαρκέσει τα θεραπευτικά του αποτελέσματα.
Έτσι, για να κάνουμε ένα φάρμακο για τον COVID-19 όπως το nirmatrelvir πιο αποτελεσματικό για μεγαλύτερη διάρκεια, πρέπει να βρούμε έναν τρόπο να επιβραδύνουμε τον μεταβολισμό του από το σώμα. Εδώ λάμπει η ριτοναβίρη:η μόνη της δουλειά είναι να μειώσει τη διάσπαση της νιρματρελβίρης, ώστε η νιρματρελβίρη να μπορεί να δράσει περισσότερο. Το ritonavir αναστέλλει το CYP3A4 , ένα κυτόχρωμα που βρίσκεται σε αφθονία στο ήπαρ που καταλύει το μεταβολισμό των φαρμάκων. Με την αναστολή της διάσπασής του, το nirmatrelvir μπορεί πλέον να αποφύγει με επιτυχία τα ένζυμα που κανονικά θα το μεταβολίζουν. Αυτό επιτρέπει στον ασθενή να βιώσει τα θεραπευτικά οφέλη του nirmatrelvir για μεγαλύτερο χρονικό διάστημα από ό,τι εάν απουσίαζε το ritonavir.
 Ένα μόριο ritonavir. Σημειώστε τους δύο θειαζολικούς δακτυλίους του κοντά στην κορυφή αυτής της εικόνας.
Ένα μόριο ritonavir. Σημειώστε τους δύο θειαζολικούς δακτυλίους του κοντά στην κορυφή αυτής της εικόνας. Τι το ιδιαίτερο έχει η δομή του ritonavir που του επιτρέπει να αναστέλλει το CYP3A4; Οι δύο ομάδες θειαζολών του! Μια θειαζόλη Η ομάδα είναι ένας ετεροκυκλικός δακτύλιος με πέντε άτομα (συμπεριλαμβανομένου του αζώτου και του θείου) και δύο διπλούς δεσμούς. Στη ριτοναβίρη, αυτές οι ομάδες θειαζολών κάνουν διπλό καθήκον υποστηρίζοντας το φάρμακο με δύο πολύ σημαντικούς τρόπους. Από δομική άποψη, κάθε δακτύλιος είναι πολύ μεγαλύτερος από τα περισσότερα άλλα συστατικά του ritonavir. Η τοποθέτηση μιας ομάδας θειαζόλης σε κάθε άκρο του μορίου αυξάνει τη συνολική σταθερότητα της ριτοναβίρης, καθιστώντας τη δομή της πιο στιβαρή.
Ο άλλος ζωτικός σκοπός της ομάδας θειαζολών είναι ότι η ριτοναβίρη αλληλεπιδρά με το CYP3A4. Το CYP3A4 περιέχει μια αίμη ομάδα που έχει άτομο σιδήρου. Το άζωτο στην ομάδα θειαζόλης της ριτοναβίρης συνδέεται στενά με αυτό το άτομο σιδήρου, οδηγώντας αυτήν την επιλεκτική αλληλεπίδραση με υψηλή συγγένεια δέσμευσης. Αυτή η δέσμευση είναι τόσο ισχυρή, στην πραγματικότητα, που είναι μη αναστρέψιμη. Τούτου λεχθέντος, το σώμα αναπόφευκτα θα μεταβολίσει τα μόρια ritonavir και nirmatrelvir τελικά. Ανεξάρτητα από αυτό, αυτή η υπερειδική και μη αναστρέψιμη δεσμευτική δράση διασφαλίζει ότι τα αποτελέσματα του φαρμάκου θα διαρκέσουν όσο το δυνατόν περισσότερο πριν συμβεί αυτό.
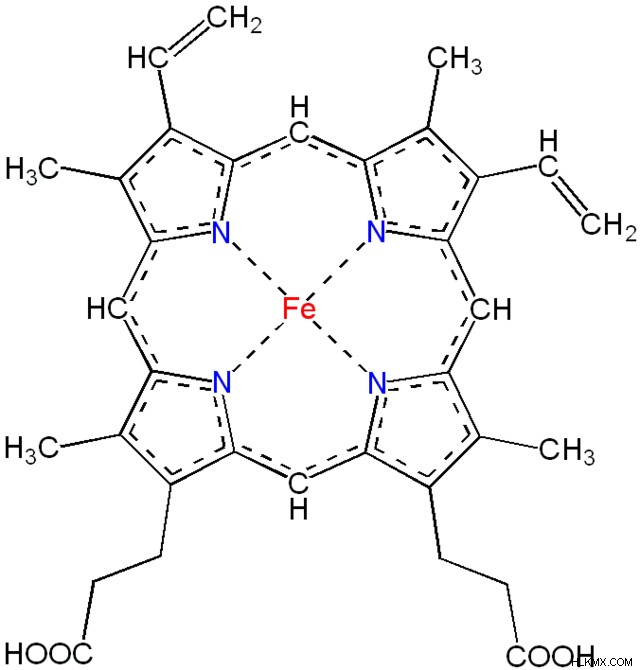 Μια επισκόπηση της δομής της ομάδας αίμης, που δείχνει το άτομο σιδήρου (κόκκινο) και τα μη εντοπισμένα ηλεκτρόνια (διακεκομμένες γραμμές). Η ομάδα θειαζόλης της ριτοναβίρης συνδέεται με τον σίδηρο για να αναστέλλει τη μεταβολική δραστηριότητα του CYP3A4.
Μια επισκόπηση της δομής της ομάδας αίμης, που δείχνει το άτομο σιδήρου (κόκκινο) και τα μη εντοπισμένα ηλεκτρόνια (διακεκομμένες γραμμές). Η ομάδα θειαζόλης της ριτοναβίρης συνδέεται με τον σίδηρο για να αναστέλλει τη μεταβολική δραστηριότητα του CYP3A4. Αγκαλιάζοντας την αλλαγή:Πώς τα προφάρμακα μετατρέπονται σε ενεργές μορφές
Τώρα, ας ξαναδούμε το lufotrelvir, τον προκάτοχο του nirmatrelvir. Όταν το lufotrelvir φτάσει στην κυκλοφορία του αίματος, το ένζυμο αλκαλική φωσφατάση το διασπά στην ενεργό του μορφή αρκετά γρήγορα. Ως εκ τούτου, το ίδιο το lufotrelvir είναι ένα προφάρμακο , ο ανενεργός πρόδρομος της δραστικής μορφής ενός φαρμάκου, που μετατρέπεται στην ενεργή μορφή in vivo . Ως ενεργή μορφή του φαρμάκου, αυτή η διασπασμένη εκδοχή του lufotrelvir είναι αυτό που έχει αντιικές λειτουργίες. Αυτό είναι βασικό για την επιτυχία της ως θεραπεία για τον COVID-19. Ευτυχώς, το lufotrelvir έχει δείξει αποτελεσματικότητα έναντι πολλών παραλλαγών — ένα πολύτιμο χαρακτηριστικό, αφού έχουμε δει πολλές φορές να μεταλλάσσεται ο ιός SARS-CoV-2.
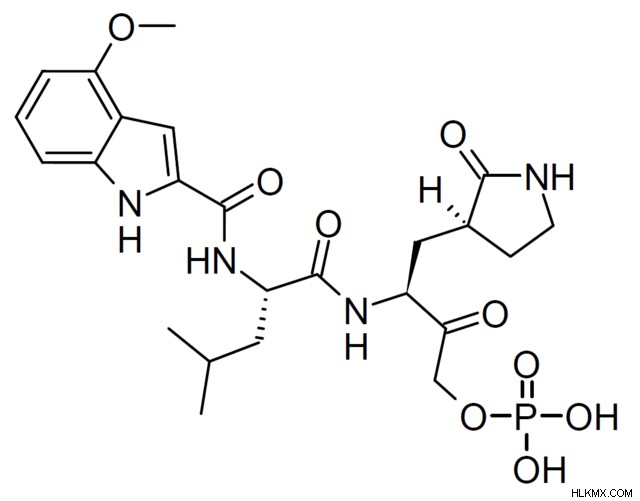 Η μοριακή δομή του lufotrelvir. Βλέπουμε ότι υπάρχει μια ομάδα φωσφορικών αλάτων όπου το nirmatrelvir έχει μια κυανό ομάδα.
Η μοριακή δομή του lufotrelvir. Βλέπουμε ότι υπάρχει μια ομάδα φωσφορικών αλάτων όπου το nirmatrelvir έχει μια κυανό ομάδα. Αρχικά, το lufotrelvir επέδειξε άτονη σταθερότητα επειδή έτεινε να επιμερίζεται. Διαμετατροπή μεταξύ επιμερών (διαστερεομερή που έχουν ένα διαφορετικό χειρικό κέντρο) μπορεί να έχουν επιπτώσεις στη βιοδραστικότητα, το μεταβολισμό και την ικανότητα ενός μορίου να αντιστέκεται στην αποικοδόμηση. Για το lufotrelvir, η τάση υποβάθμισης ήταν ένα ιδιαίτερα σημαντικό ζήτημα. Για να διορθωθεί αυτό, οι φαρμακευτικοί επιστήμονες τροποποίησαν το lufotrelvir κατά τη διαδικασία ανάπτυξης φαρμάκων. Μερικές τέτοιες τροποποιήσεις περιλαμβάνουν προσθήκη Claisen (επέκταση του μορίου με σχηματισμό δεσμού άνθρακα-άνθρακα) και φωσφορυλίωση (δημιουργώντας την φωσφορική του ομάδα). Προφανώς, αυτές οι αλλαγές άξιζαν τον κόπο. κλινικές μελέτες δείχνουν ότι το προφάρμακο μετατρέπεται στη δραστική μορφή με σχεδόν ολοκλήρωση. Όταν ένα μεγαλύτερο ποσοστό ενός φαρμάκου είναι ενεργό, το φάρμακο είναι πιο αποτελεσματικό επειδή αξιοποιεί στο έπακρο τις δαπανηρές, χρονοβόρες προσπάθειες ανάπτυξης φαρμάκων που το γέννησαν.
Θυμηθείτε ότι η διάσπαση του lufotrelvir στην ενεργό του μορφή συμβαίνει στην κυκλοφορία του αίματος. Αυτό διευκολύνεται από το γεγονός ότι το lufotrelvir χορηγείται ενδοφλεβίως, απευθείας στην κυκλοφορία του αίματος. Αφού ενεργοποιηθεί η ενεργή μορφή του lufotrelvir, το σώμα καθαρίζει το φάρμακο μέσω της υδρόλυσης αμιδίου, μια μεταβολική διαδικασία που θα δούμε περισσότερα σύντομα. Μέχρι στιγμής, έχουμε μάθει πολλά για το τι κάνουν τα φάρμακα για τον COVID-19 μόλις εισέλθουν στο σώμα. Στη συνέχεια, θα κάνουμε ένα βήμα πίσω και θα εξετάσουμε ένα θέμα στο οποίο έχουμε αναφερθεί:πώς αυτά τα φάρμακα εισέρχονται στον οργανισμό αρχικά.
Οι περιπλοκές της παράδοσης φαρμάκων
Το Nirmatrelvir και το πρόδρομο μόριο του lufotrelvir συνδέονται στενά, αλλά έχουν κάποιες σημαντικές διαφορές. Από αυτά τα δύο φάρμακα, το nirmatrelvir (όταν συνοδεύεται από την ένωση ritonavir) είναι γενικά η προτιμώμενη θεραπευτική επιλογή επειδή μπορεί να χορηγηθεί ως χάπι. Αντίθετα, το lufotrelvir μπορεί να χορηγηθεί μόνο ενδοφλεβίως, γεγονός που το καθιστά λιγότερο βολικό εναλλακτικό.
Το πώς ένας ασθενής καταναλώνει ένα φάρμακο έχει σημασία. Τα χάπια είναι βολικά για τους ασθενείς επειδή είναι φορητά, έχουν ήδη χωριστεί σε κατάλληλες δόσεις και ο ασθενής μπορεί να πάρει κάθε δόση χωρίς να χρειάζεται να είναι παρών ο πάροχος υγειονομικής περίθαλψης (HCP). Η ευκολία είναι ένα πολύ επιθυμητό χαρακτηριστικό σε ένα φάρμακο, όχι μόνο από την πλευρά του ασθενούς, αλλά και από την οπτική γωνία του HCP. Ένας ασθενής είναι πολύ πιο πιθανό να συνεχίσει τη λήψη ενός φαρμάκου και να το πάρει ακριβώς όπως έχει συνταγογραφηθεί, εάν είναι βολικό να το κάνει. Σε τελική ανάλυση, η συνταγογράφηση ενός φαρμάκου δεν αξίζει ούτε για τον ασθενή ούτε για τον χρόνο του HCP, εάν ο ασθενής δεν χρησιμοποιήσει σωστά αυτό το φάρμακο και δεν επωφεληθεί από τα αποτελέσματά του.
Το κύριο μειονέκτημα ενός χαπιού είναι ο χρόνος που απαιτείται για να δράσει. Όταν καταναλώνετε ένα χάπι από το στόμα, περνά από το πεπτικό σας σύστημα:το οξύ του στομάχου σας το διασπά και στη συνέχεια τα έντερά σας το απορροφούν. Αυτή η διαδικασία είναι αβίαστη από την πλευρά του ασθενούς, αλλά απαιτεί χρόνο. Ως υποπροϊόν, υποβάλλει επίσης τις ενώσεις του φαρμάκου σε βιοχημική αποσύνθεση — ας διερευνήσουμε πώς.
Βιοδιαθεσιμότητα και σταθερότητα φαρμάκων
Σε κάθε στροφή του πεπτικού συστήματος, αυτές οι ενώσεις συναντούν και αλληλεπιδρούν με πεπτικούς παράγοντες όπως τα ένζυμα. Μέσω χημικών αντιδράσεων και μεταβολικών λειτουργιών, αυτά τα ένζυμα μπορεί να τροποποιήσουν τις λειτουργικές ομάδες στις χημικές δομές των ενώσεων, αποκλίνοντάς τες από αυτό που σκόπευαν οι βιοϊατρικοί ερευνητές. Εάν αυτό συμβεί πριν ο οργανισμός απορροφήσει το φάρμακο, τότε το φάρμακο θα είναι λιγότερο αποτελεσματικό συνολικά. (Εάν σας είπαν ποτέ να πάρετε ένα χάπι με ή χωρίς φαγητό, αυτός είναι ένας από τους λόγους! Το σώμα μπορεί να απορροφήσει ορισμένα φάρμακα πιο αποτελεσματικά ή λιγότερο αποτελεσματικά, ανάλογα με το εάν υπάρχει ή όχι τροφή στο στομάχι.) Μεταφρασμένα σε ένα πλαίσιο υγειονομικής περίθαλψης, αυτές οι περιστάσεις μπορεί να οδηγήσουν τον ασθενή να βιώσει λιγότερο θεραπευτικό όφελος.
Αντίθετα, τα ενδοφλέβια φάρμακα χορηγούνται απευθείας στην κυκλοφορία του αίματος, με τα αποτελέσματά τους να συμβαίνουν πολύ πιο γρήγορα από αυτά ενός χαπιού. Οποιοδήποτε ενδοφλέβιο φάρμακο, δεδομένου ότι παρακάμπτει εντελώς τη διαδικασία πέψης, δείχνει επίσης πλήρη βιοδιαθεσιμότητα. Βιοδιαθεσιμότητα μετρά το ποσοστό ενός φαρμάκου που φτάνει στο κυκλοφορικό σύστημα, άρα τα ενδοφλέβια φάρμακα έχουν (θεωρητική) βιοδιαθεσιμότητα 100%. Τα χάπια παρουσιάζουν χαμηλότερη βιοδιαθεσιμότητα επειδή, λόγω της πεπτικής διαδικασίας, ένα μέρος του φαρμάκου θα χάνεται πάντα στον μεταβολισμό του σώματος. Οι επιστήμονες μετρούν τη βιοδιαθεσιμότητα ως δείκτη της διάρκειας ενός φαρμάκου. Με υψηλότερη βιοδιαθεσιμότητα, ένας ασθενής θα αισθάνεται ότι τα αποτελέσματα μιας εφάπαξ δόσης επιμένουν περισσότερο σε σύγκριση με ένα φάρμακο με χαμηλότερη βιοδιαθεσιμότητα. Επομένως, ο τρόπος χορήγησης ενός φαρμάκου έχει διαφορά στο πώς το βιώνει ο ασθενής και για πόσο καιρό. Η χρήση τυποποιημένων μετρήσεων όπως η βιοδιαθεσιμότητα προσθέτει στη συζήτηση, επιτρέποντας στους ερευνητές να κάνουν δίκαιες συγκρίσεις μεταξύ πολύ διαφορετικών φαρμάκων.
Εάν ένα φάρμακο είναι διαθέσιμο και σε μορφή χαπιού και σε ενδοφλέβια μορφή, κάθε μορφή χρησιμοποιεί διαφορετική δοσολογία. Αυτό αντισταθμίζει τις διαφορές στη βιοδιαθεσιμότητα των μορφών. Μέχρι τώρα, γνωρίζουμε ότι λιγότερο από το φάρμακο καταφέρνει να φτάσει στο κυκλοφορικό σύστημα όταν το φάρμακο είναι ένα χάπι. Όταν το φάρμακο χορηγείται ως χάπι, χορηγείται σε υψηλότερη δόση σε σύγκριση με όταν χορηγείται ενδοφλέβια. Είναι προφανές εδώ ότι η βιοδιαθεσιμότητα σχετίζεται άμεσα με παράγοντες όπως η μορφή χορήγησης του φαρμάκου, το επίπεδο δοσολογίας και η χορήγηση.
Λάβετε επίσης υπόψη σας ότι παίζουν και άλλοι λεπτοί παράγοντες. Για παράδειγμα, σε έναν πληθυσμό ασθενών, οι ερευνητές βλέπουν μεμονωμένες διαφορές στο πόσο γρήγορα και πόσο ένα φάρμακο απορροφάται από κάθε ασθενή. Σε κάποιο βαθμό, οι ερευνητές κατανοούν ότι η απορρόφηση του φαρμάκου εξαρτάται από στοιχεία όπως η ώρα της ημέρας που λαμβάνεται το φάρμακο, το βάρος και το βιολογικό φύλο του ασθενούς και πολλά άλλα. Όμως, όταν σχεδιάζουν ένα φάρμακο, οι ερευνητές δεν μπορούν να λάβουν πλήρως υπόψη όλες τις μεταβλητές ιδιοσυγκρασίες που θα μπορούσαν να επηρεάσουν την απορρόφηση. Αντίθετα, προσπαθούν να σχεδιάσουν ένα φάρμακο που να λειτουργεί για την πλειοψηφία των ασθενών με τρόπο ασφαλή, προβλέψιμο και όσο το δυνατόν πιο αποτελεσματικό.
Όλες αυτές οι σκέψεις εμπλουτίζουν τις συζητήσεις γύρω από τη σταθερότητα των φαρμάκων. Στα φαρμακευτικά προϊόντα, σταθερότητα αναφέρεται στην ικανότητα ενός φαρμάκου να διατηρεί σταθερές ιδιότητες από τη στιγμή που παρασκευάζεται μέχρι τη στιγμή που το χρησιμοποιεί ο ασθενής. Η αξιολόγηση της σταθερότητας ενός φαρμάκου πραγματοποιείται σε συνεχή βάση, τόσο εντός όσο και εκτός του σώματος του ασθενούς. Για παράδειγμα, οι φαρμακευτικοί ερευνητές θέλουν να διασφαλίσουν ότι ένα φάρμακο είναι σταθερό στο ράφι, διατηρεί αξιόπιστα την ποιότητα και την αποτελεσματικότητά του μέχρι την ημερομηνία λήξης του και έχει σημαντική επίδραση στην υγεία του ασθενούς μετά την κατανάλωσή του. Η χαμηλότερη σταθερότητα υποδηλώνει ότι ένα φάρμακο δεν θα λειτουργήσει τόσο καλά όσο προορίζεται για όσο διάστημα προβλέπεται. Αυτό θα μπορούσε να έχει βαθιές συνέπειες για τους ασθενείς, οι οποίοι προφανώς αναμένουν ότι τα φάρμακά τους θα λειτουργήσουν σωστά.
Οι διαφαινόμενες απειλές της οξείδωσης και της υδρόλυσης
Δύο παραδείγματα χημικών αντιδράσεων που απειλούν συνήθως τη σταθερότητα του φαρμάκου είναι η οξείδωση και η υδρόλυση. Οξείδωση αντιδράσεις, όπου χάνονται ηλεκτρόνια, μπορεί να συμβούν με την πάροδο του χρόνου εκθέτοντας το φάρμακο σε συνθήκες όπως το φως ή η θερμότητα. Για να αποφευχθεί η υποβάθμιση, οι κατασκευαστές παρέχουν συγκεκριμένες οδηγίες για την αποθήκευση του φαρμάκου:σε ποιες θερμοκρασίες, πόση προστασία από το φως κ.λπ. Απλώς σκεφτείτε πόσες χημικές αντιδράσεις εξαρτώνται από το πώς μια ένωση κλέβει, ανταλλάσσει, χάνει ή κερδίζει τα ηλεκτρόνια ενός άλλου μορίου. Εάν η οξείδωση συμβεί πρόωρα λόγω εσφαλμένων συνθηκών αποθήκευσης, η χημική δομή του φαρμάκου θα έχει διαφορετικό αριθμό ηλεκτρονίων από αυτόν που θα έπρεπε, επομένως δεν θα υποστεί αυτές τις αντιδράσεις με τυπικό τρόπο. Σε ορισμένες περιπτώσεις, αυτό μπορεί να κάνει το ίδιο το φάρμακο να μην λειτουργεί όπως θα έπρεπε.
Η απλή τήρηση των οδηγιών αποθήκευσης του κατασκευαστή του φαρμάκου μπορεί να ελαχιστοποιήσει την πιθανότητα οξείδωσης. Αλλά εκτός από την οξείδωση, μια πιο συχνά παρατηρούμενη οδός για την αποσύνθεση ενός φαρμάκου είναι η υδρόλυση. Υδρόλυση περιλαμβάνει τη χρήση νερού για τη διάσπαση του χημικού δεσμού ενός μορίου. Ανάλογα με την αρχική δομή του μορίου, μια απλή αντίδραση υδρόλυσης μπορεί να αλλάξει εντελώς το βιοχημικό του προφίλ. Παρουσία νερού, λειτουργικές ομάδες που βρίσκονται συχνά σε φαρμακευτικά φάρμακα - εστέρες και αμίδια, για να αναφέρουμε ένα ζευγάρι - μπορεί να μετατραπούν σε ομάδες καρβοξυλικού οξέος ή αλκοόλης.
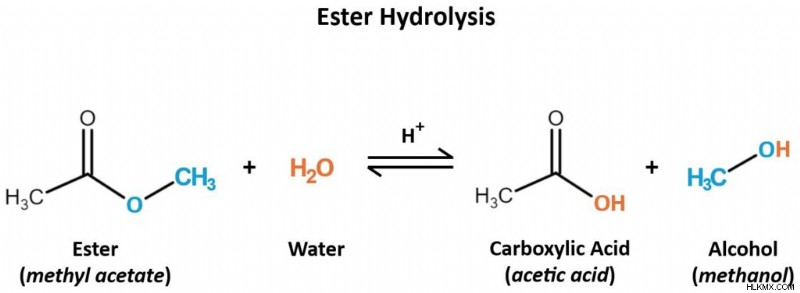 Σε όξινες συνθήκες, τα μόρια του νερού υδρολύουν μόρια εστέρα σε καρβοξυλικό οξύ και προϊόντα αλκοόλης. Αν και αυτή είναι μια αναστρέψιμη αντίδραση, έχει τη δυνατότητα να επηρεάσει τη λειτουργία ενός φαρμάκου.
Σε όξινες συνθήκες, τα μόρια του νερού υδρολύουν μόρια εστέρα σε καρβοξυλικό οξύ και προϊόντα αλκοόλης. Αν και αυτή είναι μια αναστρέψιμη αντίδραση, έχει τη δυνατότητα να επηρεάσει τη λειτουργία ενός φαρμάκου. 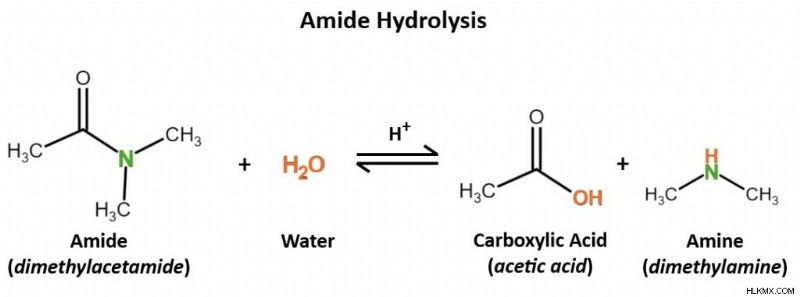 Το νερό, πάλι υπό όξινες συνθήκες, υδρολύει ένα αμίδιο για να δώσει προϊόντα καρβοξυλικού οξέος και αμίνης.
Το νερό, πάλι υπό όξινες συνθήκες, υδρολύει ένα αμίδιο για να δώσει προϊόντα καρβοξυλικού οξέος και αμίνης. Μέσα στο σώμα, η υδρόλυση συμβαίνει χάρη στα ένζυμα που βρίσκουμε σε διάφορους ιστούς. Όσο πιο γρήγορα αυτά τα ένζυμα υδρολύουν ένα φάρμακο, τόσο πιο σύντομη θα διαρκέσει η δράση αυτού του φαρμάκου. Προκειμένου να αποδοθεί το ίδιο όφελος με ένα μη υδρολυμένο φάρμακο, μπορεί να απαιτούνται συχνότερες ή υψηλότερες δόσεις. Επομένως, ένας τρόπος για να ενισχυθεί η αποτελεσματικότητα ενός φαρμάκου είναι ο σχεδιασμός του χρησιμοποιώντας λειτουργικές ομάδες που είναι λιγότερο επιρρεπείς στην υδρόλυση αρχικά.
Παρόλα αυτά, το γεγονός ότι ένα φάρμακο υφίσταται χημικές αντιδράσεις δεν είναι εγγενώς κακό. Άλλωστε, το φάρμακο πρέπει να διασπαστεί τελικά! Εάν δεν συνέβαινε, τότε τα επίπεδα του φαρμάκου θα συσσωρεύονταν συνεχώς στο σώμα και ο ασθενής μπορεί να υποφέρει από δυσάρεστες παρενέργειες όπως τοξικότητα ή βλάβη οργάνων. Αυτό που έχει σημασία είναι πώς οι ερευνητές επιτυγχάνουν τη λεπτή ισορροπία του μεταβολισμού των φαρμάκων. Στην ιδανική περίπτωση, ένα φάρμακο θα πρέπει να αντιστέκεται σε πρόωρες χημικές αντιδράσεις για αρκετό καιρό ώστε να έχει θεραπευτικό αποτέλεσμα στον οργανισμό του ασθενούς. Αφού ολοκληρωθούν αυτές οι επιδράσεις, θα πρέπει να παραδοθεί σε μεταβολικές χημικές αντιδράσεις, ώστε το σώμα να μπορεί να το αποβάλλει. Ο προσδιορισμός του πότε πρέπει να συμβεί αυτός ο μεταβολισμός είναι ένα κεντρικό ερώτημα κατά τις φάσεις ανάπτυξης φαρμάκων όπου οι ερευνητές μελετούν το φάρμακο in vivo για να κατανοήσετε πώς λειτουργεί μεταξύ των ενεργών ενζύμων, ενώσεων και ιστών του σώματος.
Ανεξάρτητα από τα μοναδικά χαρακτηριστικά τους, καθένα από τα φάρμακα για τον COVID-19 που παρουσιάσαμε σε αυτό το άρθρο λειτουργεί ως αντιιικό φάρμακο. (Psst: Ένας σίγουρος τρόπος να το καταλάβετε είναι με το «-vir» που τελειώνει σε κάθε ένα από τα ονόματά τους.) Αλλά μία από αυτές τις τέσσερις ενώσεις δεν είναι σαν τις άλλες. Το ritonavir δεν είναι απλώς ένα αντιικό φάρμακο. είναι ένα αντιρετροϊκό φάρμακο . Ας εξετάσουμε τι σημαίνει αυτό στο πλαίσιο του COVID-19.
Δημιουργία αντιγράφων ασφαλείας:Τι είναι ο ρετροϊός;
Τα αντιιικά φάρμακα στοχεύουν έναν ή περισσότερους ιούς, αλλά τα αντιρετροϊκά φάρμακα στοχεύουν ειδικά ρετροϊούς . Όταν μολύνει ένα κύτταρο ξενιστή, ένας ρετροϊός χρησιμοποιεί την αντίστροφη μεταγραφάση του ένζυμο για τη δημιουργία ενός κλώνου DNA που είναι συμπληρωματικό με το δικό του γονιδίωμα RNA. Θυμηθείτε, το κεντρικό δόγμα της βιολογίας δηλώνει ότι το DNA μεταγράφεται σε RNA, το οποίο τελικά παράγει πρωτεΐνες. Η δημιουργία DNA από RNA σημαίνει αντιστροφή της τυπικής διαδικασίας μεταγραφής. Αυτή η αλληλουχία RNA-to-DNA είναι όπου οι ρετροϊοί παίρνουν το όνομά τους. Μόλις το γενετικό του υλικό μετατραπεί σε DNA, ο ρετροϊός μπορεί να αναλάβει τον φυσικό μηχανισμό αντιγραφής του κυττάρου ξενιστή. Αυτό επιτρέπει στον ρετροϊό να αναπαράγει το γονιδίωμά του και να δημιουργεί νέα αντίγραφα του εαυτού του για τη διάδοση της μόλυνσης. Ίσως το πιο γνωστό παράδειγμα ρετροϊού είναι ο HIV-1, ο ιός πίσω από το HIV/AIDS.
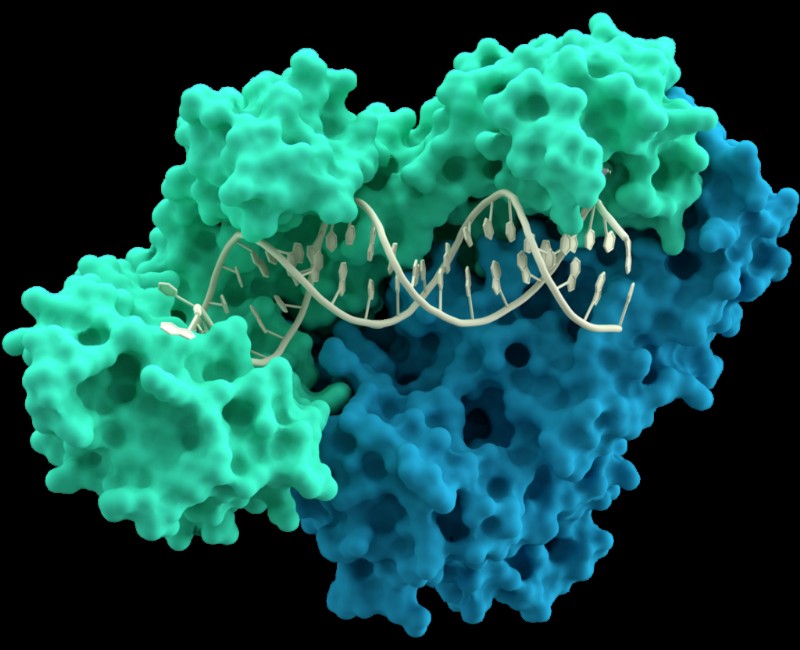 Μοντέλο υπομονάδων p66 (πράσινη) και p51 (μπλε) της αντίστροφης μεταγραφάσης που αλληλεπιδρούν με ένα μόριο DNA (εκατό).
Μοντέλο υπομονάδων p66 (πράσινη) και p51 (μπλε) της αντίστροφης μεταγραφάσης που αλληλεπιδρούν με ένα μόριο DNA (εκατό). Είναι σημαντικό να σημειωθεί ότι οι κοροναϊοί, όπως ο SARS-CoV-2, δεν είναι ρετροϊοί. Οι κοροναϊοί και οι ρετροϊοί ανήκουν σε εντελώς ξεχωριστές ταξινομικές οικογένειες. Εάν συμβαίνει αυτό, τότε γιατί μια αντιρετροϊκή ένωση όπως η ριτοναβίρη θα ήταν χρήσιμη στην καταπολέμηση του κοροναϊού;
Παρά τις διαφορές τους, υπάρχουν κάποιες σημαντικές ομοιότητες μεταξύ των ρετροϊών και των κοροναϊών. Και οι δύο χρησιμοποιούν το RNA ως γενετικό τους υλικό, παραβιάζουν τους έμφυτους μηχανισμούς των κυττάρων-ξενιστών για να αναπαραχθούν και χρειάζονται πρωτεάσες για αντιγραφή. Πρωτεάσες είναι ένζυμα που διασπούν τις πρωτεΐνες. Σε αυτήν την περίπτωση, διασπούν τις πρωτεΐνες που χρειάζεται ο ρετροϊός ή ο κοροναϊός για να αναπαραχθεί.
Το Nirmatrelvir και το ritonavir, καθώς και το lufotrelvir, είναι όλα αναστολείς πρωτεάσης . Σκοπός τους είναι να σταματήσουν τα ένζυμα πρωτεάσης που βοηθούν την εξάπλωση των ρετροϊών και των κοροναϊών. Το ritonavir ξεκίνησε στην πραγματικότητα ως θεραπεία για τον HIV-1. Κατά τη διάρκεια της πανδημίας COVID-19, οι επιστήμονες επαναχρησιμοποίησαν τη ριτοναβίρη για να μελετήσουν τον αντίκτυπό της στον SARS-CoV-2. Και, αγόρι, είχε αντίκτυπο.
Το σώμα μεταβολίζει φυσικά τους αναστολείς πρωτεάσης με την πάροδο του χρόνου, ιδιαίτερα στα έντερα και το ήπαρ. Από φαρμακευτική άποψη, αυτό σημαίνει ότι οι αναστολείς πρωτεάσης αναπόφευκτα θα διασπαστούν. Για να διαρκέσουν αυτά τα φάρμακα περισσότερο στο σώμα, μπορούμε να χορηγήσουμε ένα άλλο φάρμακο που επιβραδύνει αυτόν τον μεταβολισμό. Αυτός είναι ο λόγος για τον οποίο το nirmatrelvir, ο κύριος χαρακτήρας του Paxlovid, συνοδεύεται από ritonavir σε ένα μόνο φάρμακο. Και οι δύο είναι αναστολείς πρωτεάσης, αλλά η ριτοναβίρη έχει σχεδιαστεί ειδικά για να αναστέλλει το ένζυμο CYP3A4 που διασπά τους αναστολείς πρωτεάσης. Με άλλα λόγια, το ritonavir επιβραδύνει τις δυνάμεις που μεταβολίζουν το nirmatrelvir, επιτρέποντας στο nirmatrelvir να έχει μεγαλύτερη επίδραση στον οργανισμό. Με μειωμένη απειλή μεταβολισμού, το nirmatrelvir μπορεί να επικεντρωθεί στο να κάνει αυτό που κάνει καλύτερα:να διασπάσει τις πρωτεΐνες που επιτρέπουν τη διάδοση του COVID-19.
Η επαναχρησιμοποίηση ενός φαρμάκου τείνει να είναι ένα παιχνίδι δοκιμής και λάθους. Χρησιμοποιώντας όσα ήδη γνωρίζουν για την ασθένεια που τους ενδιαφέρει, οι ερευνητές προβλέπουν ποια υπάρχοντα φάρμακα θα μπορούσαν να δράσουν εναντίον της. Στη συνέχεια, σε εργαστηριακά περιβάλλοντα και κλινικές δοκιμές, δοκιμάζουν πόσο καλά αυτό το φάρμακο πραγματικά δρα κατά της ασθένειας ενδιαφέροντος. Εάν οι κλινικές δοκιμές είναι επιτυχείς, τότε οι ρυθμιστικές αρχές ενδέχεται να εγκρίνουν το φάρμακο για τη θεραπεία αυτής της ασθένειας.
Τι γίνεται όταν τα φάρμακα δεν δουλειά;
Μόλις ένα φάρμακο βγει στην αγορά, μπορούμε να δούμε πόσο καλά λειτουργεί πραγματικά πέρα από ένα εργαστήριο ή ένα περιβάλλον κλινικής έρευνας. Μερικές φορές, το φάρμακο λειτουργεί ακριβώς όπως προβλέπεται χωρίς ούτε έναν λόξυγκα. Άλλες φορές, ωστόσο, τα πράγματα δεν πάνε όπως είχαν προγραμματιστεί και νέα εμπόδια αποκαλύπτονται μόνο αφού το φάρμακο φτάσει σε πραγματικούς ασθενείς.
Ας το δούμε αυτό από την οπτική γωνία μιας από τις μεγαλύτερες ιατρικές απειλές της εποχής μας:της αντίστασης στα αντιβιοτικά. Αντίσταση σημαίνει ότι το παθογόνο που στοχεύει ένα φάρμακο (σε αυτή την περίπτωση, ένα βακτήριο που προκαλεί ασθένεια) σταδιακά γίνεται πιο ικανό να αντέξει αυτό το φάρμακο (το αντιβιοτικό). This has dire implications for the pharmaceutical industry, which then must devise a new bacteria-killing drug that the bacteria aren’t resistant to yet, and for the patients who suffer from incurable bacterial infections in the meantime.
Unfortunately, this phenomenon happens with protease inhibitors, too. Viruses that are normally susceptible to protease inhibitors can, over time, develop resistance to those drugs. When that happens, the protease inhibitors become less effective as antiviral medications. How does this happen in the first place?
In order to stop viral replication, a protease inhibitor must bind to a specific site on the virus’s protease. This is how protease inhibitors work under normal circumstances, as intended, to treat a viral infection. In its genome, a virus encodes the proteases that it needs for replication. But, as we know, genetic material can mutate — and any mutation can change the nature of the protease.
If a mutation changes the protease’s active site, this directly impacts its affinity for binding to the protease inhibitor. It’s possible for the active site to mutate to have a lower affinity for the drug, which limits the medication’s ability to target the protease. This is how protease inhibitor resistance arises. Without a selective target available, the protease inhibitor can’t do its job effectively, so it’s no longer a useful solution against the virus it ought to fight.
Mutations can happen spontaneously, and they tend to arise as a virus evolves over many replication cycles. This introduces a bit of a conundrum:scientists invented protease inhibitors to prevent viral reproduction, but as a result of viral reproduction itself, mutations can arise that change a protease inhibitor’s effectiveness. During the COVID-19 pandemic, we saw precisely how concerning viral evolution and mutation are, as newly-evolved mutant variants repeatedly rendered our vaccines less effective.
To overcome the challenging prospect of a protease-inhibitor–resistant virus, protease inhibitors can be used in combination with antiviral medications that have different targets. This way, even if the virus’s active site mutates to become resistant and the protease inhibitor can no longer bind there, another medication can step in to target a different structure or function of the virus instead. Spreading the virus-fighting burden across multiple diverse drug classes can help stop the virus’s spread. But wait — what’s a drug class, and what does it mean for the virus that causes COVID-19?
Class is in Session:Pinpointing the Right Medication for the Right Job
There’s no “miracle” antiviral drug that can treat every viral disease out there, but that doesn’t stop scientists from trying! Researchers group similar medications into classes based on their properties and functions. Oftentimes, these classes directly describe how the drug functions. Some familiar examples readily come to mind:drugs in the stimulant class stimulate the body or mind, contrasted with drugs of the depressant class that reduce arousal, while analgesic drugs relieve pain (the word “analgesic” comes from Greek roots that mean “without pain”).
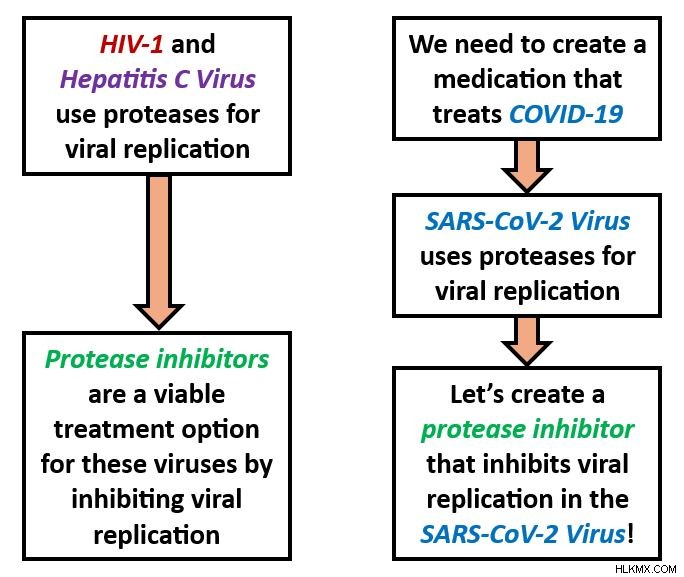
Protease inhibitors are another class of drugs that do exactly what their name implies. By inhibiting proteases, a type of enzyme that SARS-CoV-2 particles use for reproduction, protease inhibitors interrupt the viral life cycle by preventing the virus from replicating. The virus must make many copies of itself to infect new host cells, so preventing viral replication prevents the spread of COVID-19.
Researchers already applied the same concept to fighting the viruses behind HIV/AIDS and hepatitis C. Understanding the commonalities within a particular drug class makes it easy to translate existing medications into new contexts to treat different diseases. To devise an effective antiviral medication to treat COVID-19, researchers had to understand a few simple, yet essential, points. First, they learned that the SARS-CoV-2 virus uses proteases in its replication process. Second, they knew that the viruses that cause AIDS and hepatitis C also use proteases to reproduce. Third, protease inhibitors already existed as safe, effective medications for treating HIV/AIDS and hepatitis C.
From here, scientists could apply this logic in a straightforward way in order to conclude that protease inhibitors are a viable COVID-19 treatment option. If protease inhibitor drugs are already known to work against other viruses that replicate via proteases, and SARS-CoV-2 is known to replicate via proteases too, why not pursue a protease inhibitor as a COVID-19 drug?
 During drug discovery, biomedical researchers don’t always have to start from scratch. Instead, they may be able to build upon existing knowledge of which medications work well against pathogens of similar diseases. Inspired by existing drugs for HIV and hepatitis C, these logical reflections guided researchers to develop protease inhibitors for SARS-CoV-2.
During drug discovery, biomedical researchers don’t always have to start from scratch. Instead, they may be able to build upon existing knowledge of which medications work well against pathogens of similar diseases. Inspired by existing drugs for HIV and hepatitis C, these logical reflections guided researchers to develop protease inhibitors for SARS-CoV-2. In some ways, drug discovery is a very sensible process. But in practice, there are a lot of factors that threaten to get impede what ought to be a smooth, uncomplicated approach. Let’s take a look.
Challenges in Treating COVID-19
Pandemics are among the most urgent public health scenarios; time is truly of the essence. To conquer the crisis, medical experts must develop and distribute a cure faster than the disease is spreading. But we know the SARS-CoV-2 virus causes COVID-19, and viral diseases, in general, cannot be cured — only managed or treated.
Facing an incurable disease, how can we devise an effective treatment, and fast? Taking on this challenge meant overcoming SARS-CoV-2’s natural evasive characteristics, drug development roadblocks, and sociocultural factors that shaped how people interacted with COVID-19. To understand why these details had such a key impact on the pandemic, let’s evaluate them in greater depth.
Virology 101:How Viruses Evade Our Efforts to Eradicate Them
We know how to take control of stubborn viruses because we’ve managed to do it many times before. For example, you’ve likely sustained a barrage of vaccines for viral diseases like chickenpox, measles, and polio. And everyone can recite by heart the cardinal rules of flu season — stay home when you’re sick, cover your mouth when you cough and sneeze, and wash your hands often. Public health principles like these are somewhat of a tradition, and we know these rules of how to beat disease. So, what happens when we encounter a virus that doesn’t play by the rules?
What makes an effective antiviral medication?
Viruses have certain properties that can make them more difficult to target than pathogens like bacteria or parasites. First of all, there’s an ongoing scientific debate as to whether viruses are living or nonliving. Viruses have their own genetic material and, inside of a host cell, they exhibit some characteristics of life, like the ability to reproduce (viral replication ). However, viruses can’t function independently, and therefore can’t do much damage, without the help of a living host cell. Since they need living hosts’ support to execute their functions, many scientists view viruses, in and of themselves, as nonliving. This invites a unique conundrum:If something isn’t alive, is it actually possible to use medications to kill it?
As part of the drug discovery process, pharmaceutical researchers determine how their medication will impact its target (which might be a protein, antibody, gene, virus, bacterium, etc.). Many drugs work by impacting the target’s ability to function, but this might not be useful against viruses. For example, a drug that works by interfering with the target’s metabolism wouldn’t be an effective antiviral drug because viruses don’t have their own metabolic processes.
Living or not, we know that viruses are vulnerable to antiviral medications. Strong antiviral medications account for their target’s normal mechanisms and viral load. By closely studying those mechanisms — how the virus infects and moves through the body, infects healthy host cells, replicates its genetic material, and causes physical symptoms — scientists can pursue a drug that interferes with them.
Viral load refers to how much virus is present in a patient’s blood. Viral load can change over the course of an infection, and it can indicate how sick the patient is. For certain diseases, a higher viral load indicates that the patient is more contagious. Some antiviral medications are intended to reduce viral load, alleviating the patient’s infection and protecting other people from catching it. (In this way, reducing viral load is a goal of a long-term HIV treatment called antiretroviral therapy , or ART .)
What’s the Password?:How Viruses Enter Host Cells
Viruses are among the smallest biological agents. After all, they have to be, in order to penetrate host cells. Viruses usually enter host cells through receptor-mediated endocytosis , a process by which the viral particle binds to a receptor on the cell membrane and passes into the cell. When descending upon a new host cell, the virus hunts for specific receptors that will bind to proteins on its own membrane.
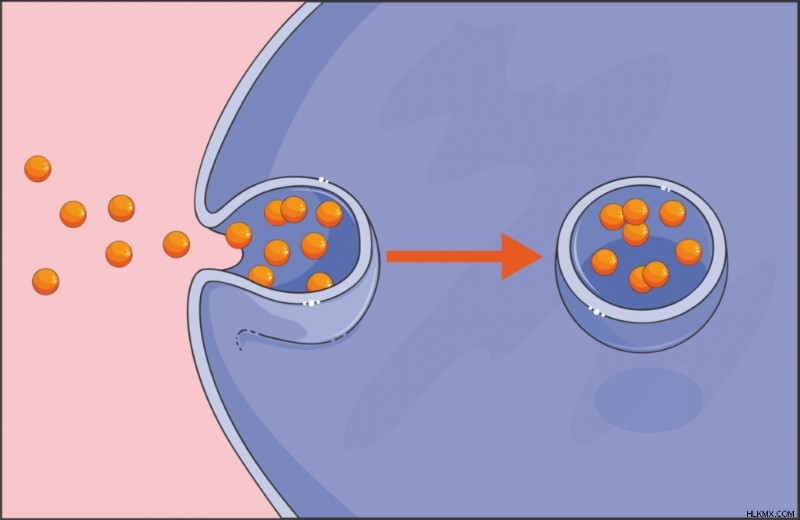 Endocytosis is a process by which particles can enter a cell. Viruses use this tactic to bind to a host cell’s membrane and invade the cell.
Endocytosis is a process by which particles can enter a cell. Viruses use this tactic to bind to a host cell’s membrane and invade the cell. This penetrative mechanism is sometimes what an antiviral drug targets. A drug that interferes with this protein’s binding to a membrane receptor prevents the virus from reaching host cells. Researchers extended this strategy to COVID-19 vaccines that notably target SARS-CoV-2’s spike protein , which binds to host cells’ ACE2 receptors. All coronaviruses have spike proteins, but the protein’s chemical makeup can fluctuate across different viral variants. This is why scientists continuously produced COVID-19 vaccines:each new version of the vaccine targeted the spike protein’s latest disguise. We already knew about coronaviruses before COVID-19 happened, but developing a COVID-19 medication required learning about the special intricacies of SARS-CoV-2’s spike protein in particular.
For being such tiny agents, viruses sure put up a big fight. A drug spurs the body to act upon a virus, but this could inadvertently lay the groundwork for further harm. In order to damage viruses, antiviral treatments must also damage the host cells that those viruses occupy. This can have further implications for the health of the patient or the symptoms that they experience. Therefore, antiviral treatments represent a balancing act, selective toxicity , between destroying the virus and preserving the patient’s own tissues.
Unfortunately, there’s no easy solution to this dilemma. Any step in the viral life cycle would be a good target for an antiviral drug, but the host cell would probably also suffer. Some antivirals reduce the risk to the patient’s health by targeting a virus-specific molecule or behavior, leaving the host cells relatively untouched. That’s the inspiration behind COVID-19 drugs like nirmatrelvir/ritonavir. Nirmatrelvir/ritonavir inhibits a protease that SARS-CoV-2 uses for replication, which prevents the virus from reproducing. (Other COVID-19 medications, like remdesivir , disrupt the replication process by introducing steric hindrance as the virus replicates its RNA. This steric hindrance stands in the way of RNA replicating to completion, putting a pause in the viral life cycle and the SARS-CoV-2 virus at a loss.)
With antiviral drugs, researchers must weigh the benefit of weakening the virus against the risk of weakening host cells. An antiviral medication that preserves a patient’s infected cells would be an ingenious discovery and a very promising treatment option — something to consider next time you find yourself bored in the lab!
Playing the Long Game
Recall from our previous article that public health professionals use epidemiological surveillance to track disease outbreaks on a population scale. We can extend this concept to a much smaller scale:detecting microscopic viruses within the body. Their minute size isn’t the only characteristic that can make viruses hard to detect. Some viruses are pros at staying inconspicuous for extended periods of time. During these periods, the virus in question may not cause obvious symptoms (or if so, the symptoms may be nonspecific). It may even fail to appear on test results.
Sometimes observed in viral infections like HIV, Epstein-Barr virus, and hepatitis, this phenomenon is a latency period. Latency periods happen when the virus is dormant for spans of weeks, months, years, or even decades. Dormancy means that the virus has infected a host, but isn’t actively replicating, or it’s replicating very slowly. Remember, for the infection to spread within the body, or from an infected to healthy person, the virus must replicate. The act of replication kills the host cell. Then, in the aftermath of cell death, the progeny from that replication seek new host cells and spread the infection.
Although certain viruses share some resemblances, like these particular viruses’ ability to stay surreptitious for long-term periods, viruses overall demonstrate very diverse features. For instance, SARS-CoV-2’s genome is composed of RNA, but many viruses’ genomes are made from DNA just like ours. Different viruses also boast different physical properties, replication techniques, and thrive in a range of environmental conditions. Maybe you can’t disrupt the virus’s life cycle, but can you do something to make its environmental conditions less hospitable? In light of such diverse traits, making antiviral medicines might seem like a fruitless pursuit, but keep in mind that every new trait presents a new angle to attach the virus.
Identifying a given virus’s individual idiosyncrasies helps researchers tailor a medication perfectly to that virus — but also means that most antiviral medications can only treat one or a handful of viruses. This lies in stark contrast to broad-spectrum antibiotics , which target numerous bacterial species. Not all antibiotics are broad-spectrum, but this all-encompassing quality is hard to replicate in antiviral drugs. Broad-spectrum antivirals do exist, but because viruses evolve so rapidly, the best antivirals would be able to defeat multiple existing strains while anticipating future variants, which is essentially a guessing game. A good place to start is with antivirals that target entire families of viruses, like coronaviruses or herpesviruses for example, that attack a stable characteristic which all of the family members have in common. Yet another example of how the shared features among different pathogens serve as the groundwork for building a single drug that fights all of them!
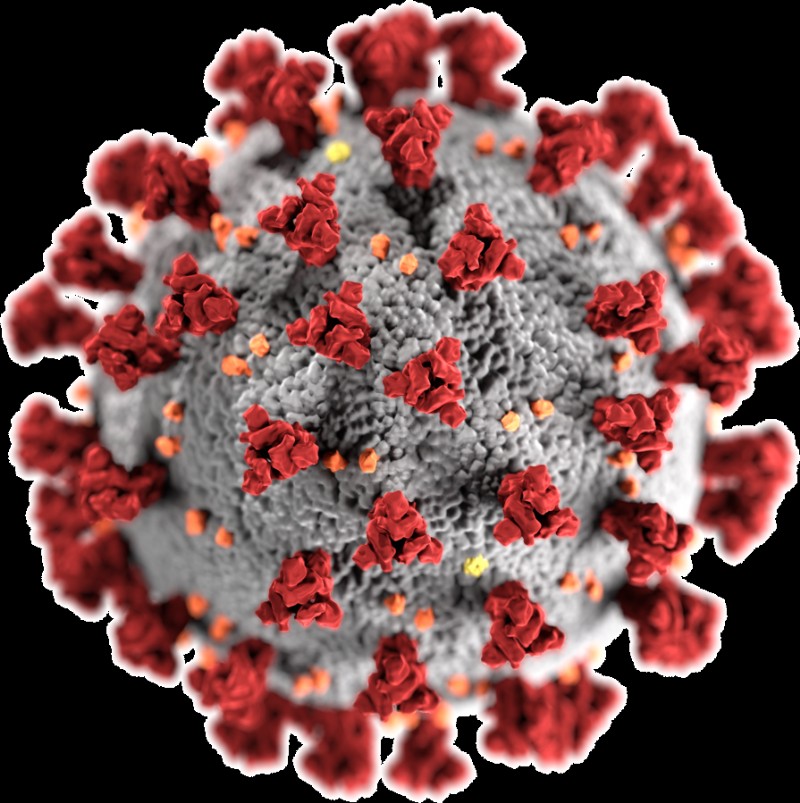 Spike proteins (red) on a SARS-CoV-2 particle project outward to readily bind with ACE2 receptors on a host cell’s membrane.
Spike proteins (red) on a SARS-CoV-2 particle project outward to readily bind with ACE2 receptors on a host cell’s membrane. Ready, Aim, Fire! All about Drug Targets
Earlier, we discussed how protease inhibitors bind with proteases that the SARS-CoV-2, HIV-1, and hepatitis C viruses encode. Recall that this binding happens selectively, and directly leads to the inhibition of viral replication. In pharmaceutical terms, we describe this dynamic dance as the protease inhibitor targeting a particular binding site on the protease. Alternatively, we can say that the protease (more specifically, the binding site) is the target of the protease inhibitor medication. But why do medications need to have targets at all?
Drugs with Multiple Targets
Most drugs need specific targets in order to treat a particular condition. But there are indeed some drugs, like certain anti-inflammatory medications and chemotherapy treatments, that target the body as a whole. This broad approach, polypharmacology , involves one drug affecting multiple targets. Anti-inflammatory drugs reduce inflammation by acting on prostaglandins — lipids that are present all over the body. And just think of the vast array of side effects that accompany chemotherapy (fatigue, nausea, hair loss, and more). The fact a single drug causes side effects that are so different from one another, which impact different systems within the body, indicates that the drug is acting on several distinct targets.
Considering the meticulous effort that goes into seeking and identifying precise targets during the drug discovery process, it might sound surprising that scientists purposely design some medications to have many targets. But for diseases such as cancer, whose wide-ranging warpaths can span multiple organs and pose a risk to the body overall, having a less specific set of targets might be the ideal solution. Each affected organ is unique, with its own profile of cell types, enzymes, and functions. The goal here is to give patients a better chance of beating a whole-body disease with a drug whose targets live throughout the whole body.
Depending on the nature of the disease, a drug’s ability to target many molecules may be either advantageous or disadvantageous.
Drugs with One Target
Let’s face it:it’s hard to maintain this big-picture outlook when working with such tiny molecules! We saw from the protease inhibitor discussion that a single binding site in the target (and sometimes a single mutation within a single binding site) can make all the difference as to whether a medication flourishes or flounders. What muddles this problem even further is the fact that a target can have multiple domains that serve as binding sites, or two very different types of molecules could have similar binding sites that interact with the drug. How do pharmaceutical researchers make a drug that acts on one binding site of interest, while ignoring all the others?
For drugs that target only one molecule, the binding interactions between the medication and its target are extremely specific. That’s an understatement! This high specificity minimizes the risk of off-target effects that can have unpleasant or dangerous consequences on the patient’s health. Designing an effective drug that has one, and only one, target requires a deep understanding of binding affinity and the structural qualities that govern it.
Remember that the drug and the target each boast a chemical structure that’s full of functional groups. Each functional group has distinctive properties that influence its reactivity, behavior, and interactions with other molecules. This means that structural characteristics lie at the core of the drug-target binding, and therefore at the core of drug effectiveness. By manipulating the functional groups in the drug’s molecular backbone, researchers can manipulate the reactions that the drug undergoes, as well as its propensity to bond with a specific domain on the target. It’s astonishing that changing out even one little atom could introduce a different a functional group and, by extension, impact a medication’s ability to work properly! Even if the drug’s functional groups stay the same, a minor change in their spatial arrangement might completely change the medication’s function.
Consider enantiomers :molecules whose structures are mirror images. One notorious case of this chirality making or breaking a medication is thalidomide. Thalidomide is a drug that was originally marketed as a morning sickness remedy. It exists as two enantiomers:the R enantiomer has a sedative effect that alleviates symptoms like morning sickness, while the S enantiomer can cause birth defects. The only chemical difference between these two drastically different outcomes is how these molecules’ atoms are spatially arranged. To make matters worse, thalidomide can interconvert its enantiomers in vivo , so even if a patient were only administered the relatively harmless R enantiomer, the teratogenic S enantiomer may arise in the body afterwards. By contrast, medications that only exist as one enantiomer, as opposed to a racemic mixture, are enantiopure drugs.
Another example of a more-than-microscopic structural change having a larger-than-life impact is the methamphetamine molecule. Methamphetamine is a stimulant and recreational drug, with side effects like vasoconstriction and rapid breathing. Its optical isomer levmetamfetamine, meanwhile, serves as a nasal decongestant of all things! Again, we see that one small switch in these drug molecules’ atomic arrangements leads to wildly different health effects.
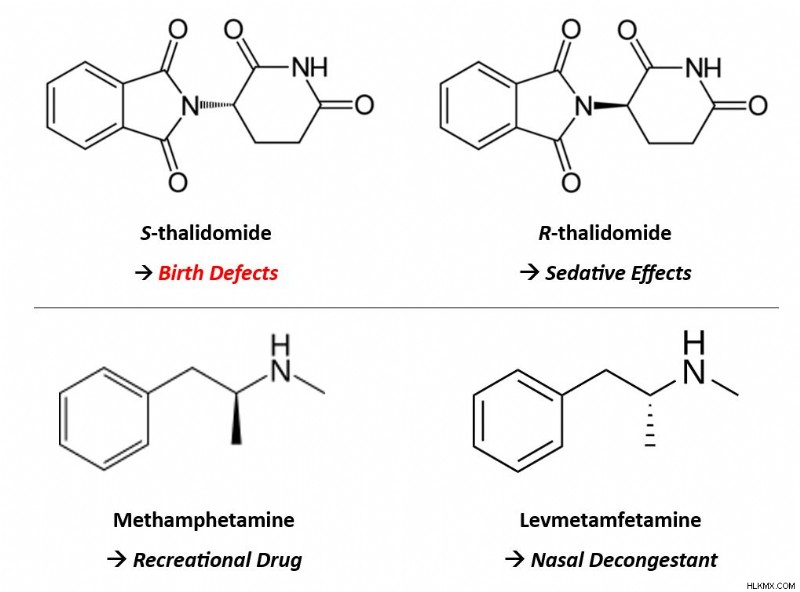 Though the only difference between each of these sets of enantiomers is the spatial arrangement of their atoms, their ensuing medical effects differ greatly.
Though the only difference between each of these sets of enantiomers is the spatial arrangement of their atoms, their ensuing medical effects differ greatly. A recurring notion in drug development is that medications are intended to be as safe and effective as possible. However, no medication can be 100% safe nor 100% effective. No matter what, there’s always the risk of side effects, off-target effects, and unwanted interactions. Regardless, scientists can maximize safety and effectiveness by tailoring a drug’s chemical properties, like its structure and functional groups, to be as specific as possible to the target of interest.
Unfortunately, achieving that specificity can be an intense challenge, especially when only one target is desired. But when different pathogens employ the same biochemical processes or enzymes as each other — like how SARS-CoV-2, HIV-1, and hepatitis C virus all employ proteases for replication — these features serve as a good starting point for drug design. Could that common feature potentially function as the drug’s target? And since several pathogens share that feature, could the drug therefore be effective against all of the pathogens? For viruses in particular, all viruses must replicate because replication is the only way viral diseases can spread to new hosts. That’s why popular COVID-19 medications target molecules, like proteases, that have a central role in SARS-CoV-2 replication. (The same is true for the protease inhibitor drugs that treat HIV and hepatitis C infection.)
Here, we’ve seen that slight changes in the drug molecule yield big impacts on its ability to bind selectively with its target (or targets). Later, we’ll talk about another highly-specific mechanism in combating disease:the interactions between antibodies and antigens. For now, let’s dive into the question of why COVID-19 medications were unusually difficult to make.
Drug Development under Dire Circumstances
The small but significant principles that we’ve mentioned so far — the fact that antibiotics don’t work against viruses, the puzzle of creating a new medication based on clues from existing ones, the arduous task of designing a drug with meaningful targets — only complicated the hunt for efficacious COVID-19 medications. Numerous additional factors were already at play, presenting challenges for drug development during a time when we needed it most.
Some of these challenges ran deep. Hardening travel restrictions and heightened political tensions, for example, strained the pharmaceutical supply chain at its core. Patients often rely on drugs manufactured elsewhere in the world, but temporary limits on international travel jeopardized typical medication supply. Worth noting is that most active pharmaceutical ingredients (APIs ), the component of a drug that gives it its therapeutic effect, are manufactured outside of the U.S. This includes being manufactured in countries that the pandemic hit hard, such as China. Importing drugs and APIs — and exporting American medicines to patients around the world — normally happens in a steady stream that ensures patients everywhere can receive their treatments when they expect to. With the short-term closures of pharmaceutical facilities and chemical plants domestically and abroad, this promise went unfulfilled in many cases. Even a brief pause in drug manufacturing can ripple into long-lasting consequences for patients.
 Pandemic-related travel restrictions hindered international drug distribution, preventing some medicines from reaching patients when expected.
Pandemic-related travel restrictions hindered international drug distribution, preventing some medicines from reaching patients when expected. Other points in the drug development process were interrupted, too. The Food and Drug Administration (FDA ), the American pharmaceutical regulatory agency, also monitors pharmaceutical sites in foreign countries. These inspections confirm that U.S.-bound drugs comply with the same rigorous safety and quality standards as those made in America. International travel restrictions, again, delayed these investigations. Inspections must happen before any medications get distributed, so from a patient perspective, postponed inspections equates to postponed treatment.
The COVID-19 pandemic struck all steps in the pharmaceutical supply chain:manufacturing, production, approval, distribution, and everything in between. This highlighted glaring vulnerabilities in this industry’s very framework, and those vulnerabilities’ effects on patients. We expect pandemics to arise occasionally, but we can’t predict when, and no two disease outbreaks are the same. That aspect of “unexpectedness” makes it extra hard to accommodate them when they do happen. Even more urgently, it underscores the need to make our drug development processes more resilient against health emergencies like pandemics. Let’s take a moment to see what that impact looks like in the context of pharmaceutical research.
A Logistical Nightmare
As soon as the World Health Organization classed COVID-19 as a pandemic, the clinical research sector scrambled to accommodate this. Mounting concerns over a mysterious disease abruptly brought many clinical trials to an indefinite pause. By the time a clinical trial starts, the researchers have already carefully planned and committed to its study protocol. During COVID-19, social distancing guidelines forced them to reimagine studies in virtual formats when possible, and postpone them when not. Trials that hadn’t begun yet were hit even harder. The number of prospective study participants plummeted as they feared COVID-19 exposure in the medical facilities where trials often occur. Some studies couldn’t even get off the ground, but those that could suddenly found themselves stuck in midair.
What’s the problem with putting a clinical trial on pause? It’s not as simple as picking up where the study left off a few weeks afterward. Surprisingly, a lot can happen in the span of a few weeks. If study participants have already received a trial dose of the drug candidate, they might experience new side effects. Researchers need to monitor these complications closely to document and address them, and to ensure the drug’s safety. Ongoing communication is paramount during trials by ensuring patients understand the nature of the study and can express their concerns. Anything that interferes with these open lines of communication, like a brutal pandemic, potentially puts the patient’s safety at risk.
During this frantic period, coronavirus clinical trials took center stage as new COVID-19 medications, therapeutics, and vaccines evolved. A large portion of biomedical research funding, media attention, and public health efforts were diverted to these studies. There’s nothing inherently bad about this, but COVID-19 wasn’t the only disease that needed trials at the time. Pausing routine studies in favor of COVID-19 trials means neglecting, at least temporarily, patients who have other medical conditions. The timing was unlucky, but other diseases didn’t cease to exist just because the pandemic happened. Striking this balance given a wide pool of patients in need, and redirecting funding appropriately, was a big challenge as COVID-19 cases skyrocketed. It even represents complex bioethical questions:How “worth pursuing” is a particular disease compared to others? Is it even possible to “rank” the value of different diseases? Who gets to determine this value?
Among the most unsettling outcomes of the pandemic is that it brought our health care infrastructure’s flaws to light. Many individuals, especially practitioners and patients who experience the health care system firsthand, were already acutely aware of its shortcomings. But COVID-19 exposed these imperfections and made them impossible to ignore. Already stretched thin, medical staff and facilities didn’t have adequate support or resources during intense waves of COVID-19 variants. Issues surrounding health equity, like overcoming health disparities and ensuring accessibility to drug treatments, became serious problems for some patients. These problems predated COVID-19 and aren’t unique to it, but the pandemic certainly emphasized them. As we determine a path forward in a post-pandemic world, public health experts think deeply about how to solve problems like these, to help everyone pursue their healthiest self.
 Resolving a pandemic extends beyond drug development. Health care personnel, regulatory employees, policymakers, and public health experts each have a key role in coordinating an effective pandemic response.
Resolving a pandemic extends beyond drug development. Health care personnel, regulatory employees, policymakers, and public health experts each have a key role in coordinating an effective pandemic response. The COVID-19 Treatment Toolbox
So far, we’ve covered two types of antiviral COVID-19 medications in detail. That’s not the whole story, though. There are other COVID-19 antiviral drugs too, and pharmaceutical treatments aren’t limited to pills either. In this section, we’ll see how the pandemic employed a multitude of other forms of treatment, even making use of the body’s natural defense mechanisms.
Monoclonal Antibodies
Even when it’s combating an infection like COVID-19, the immune system is a very powerful force. A relentless soldier in the battle for your health, its most intrinsic mission is to protect you, and it’s determined not to give up. To achieve this goal, the immune system utilizes its diverse range of physiological intricacies, some of which researchers don’t fully understand yet. Immunologists do understand the basic mechanism of how it works, though.
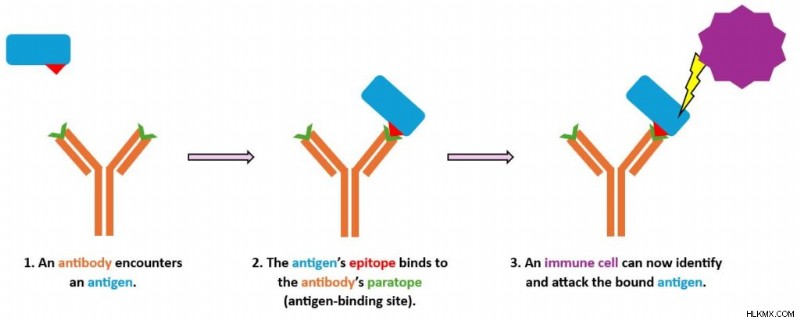
When a foreign pathogen, like the SARS-CoV-2 virus, infects you, we call that pathogen an antigen . The immune system recognizes antigens as invaders and mounts an immune response to ambush them. Among other biochemical battalions, it deploys antibodies. Antibodies are proteins made by the body’s B cells that selectively bind to antigens like a key fitting a lock. Binding is a way of flagging the antigen so other immune cells can identify, attack, and neutralize or kill it. As a component in pharmaceutical treatments, antibody therapy is an auspicious option for patients whose bodies can’t mount a sufficient immune response on their own.
How do monoclonal antibodies work?
We can classify antibodies into two broad categories. Monoclonal antibodies (mAbs ) are antibodies that target a single antigen. They’re man-made in the lab by cloning a single lineage of B cells, hence the name. By contrast, polyclonal antibodies (pAbs ) derive from multiple immune cells, arise naturally in the body in response to an infection, and can target multiple antigens.
We usually discuss mAbs as an immunotherapy in the context of cancer, where the “antigen” that they recognize is a protein on the surface of a cancer cell. More recently, their applications have extended to other conditions, including COVID-19. (Another pharmaceutical lingo lesson:a drug whose generic name ends in “-mab” is a type of monoclonal antibody.) When administered to patients, mAbs stimulate the immune system and can improve their chances of fighting off an infection. Creating mAbs in laboratories is an opportunity to precisely tailor them to a specific condition, which can enhance patient outcomes. Pharmaceutical scientists can mass-produce them with high consistency, and off-target effects are relatively unlikely because the mAb binds to only one antigen.
How does that binding make the magic happen? Given its Y-like shape, an antibody has two arms that branch off from its body (the Y’s vertical stem). On the end of each arm is a paratope , the region that binds directly to an antigen. The antigen itself features a region called an epitope . The antibody’s paratope and antigen’s epitope are extremely specific to each other. Consequently, the molecules bind together in a selective and precise manner, like a lock and key. Once the antibody has latched on to the antigen, the immune system can take action to attack that antigen.
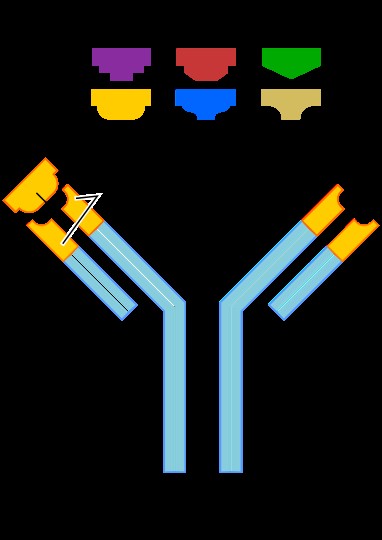 Antigens come in all shapes and sizes, but only a specific antigen can bind to a given antibody’s antigen-binding site (paratope).
Antigens come in all shapes and sizes, but only a specific antigen can bind to a given antibody’s antigen-binding site (paratope). Over time, researchers have found that COVID-19 mAbs can have different levels of effectiveness against certain SARS-CoV-2 variants. COVID-19 mAbs tend to have a harder time fighting off recent variants compared to older ones. As the pandemic evolved, novel variants dominated new infections, and some variants even showed resistance against COVID-19 treatments. It quickly became evident that antibody therapy alone, though a valuable aid, wouldn’t be a long-term solution to COVID-19.
Newly-produced antibodies travel from the B cell (a white blood cell) to the antigen’s location via the patient’s blood plasma. Everyone has blood plasma, but COVID-19 patients may be able to supplement their treatment with convalescent plasma. Next, we’ll see what that means and why it matters.
Convalescent Plasma
We just described how an infection engages the body’s immune response, including increasing the amount of antibodies in the blood. We also mentioned that the immune system’s B cells naturally produce polyclonal antibodies during an infection.
In patients who survive the infection, those antibodies don’t disappear after their symptoms clear up. As the infection resolves, the antigens in the body dwindle. But just in case these antigens dare to show their face around these parts again (in other words, if the patient were to contract the virus again in the future), these antibodies remain in the body, lying in wait to flag them for removal.
Therefore, people who have survived COVID-19 still have COVID-19 antibodies in their blood plasma. Plasma is the part of blood that excludes blood cells and platelets. Survivors can donate this blood plasma, and HCPs then process it and transfuse it into the veins of patients who are actively sick. This was a big deal during the first phase of the pandemic, before researchers managed to make a vaccine that teaches the body’s immune system to create COVID-19 antibodies. And once the vaccines were available, vaccinated folks could donate their antibody-rich plasma to COVID-19 patients even if they’d never actually had an infection themselves.
 Donor blood processing removes components like red blood cells, which is why plasma isn’t red in color.
Donor blood processing removes components like red blood cells, which is why plasma isn’t red in color. Plasma therapy is viable particularly for immunocompromised patients, who may not be capable of launching robust immune responses without it. It’s a great way for COVID-19 survivors to pay it forward and play a personal role in helping current patients. Plasma therapy is useful due to its potential to shorten the duration or severity of infection. In 2020, when no feasible COVID-19 medications were available, having ready-made antibodies in our arsenal was practical and priceless.
Making the Most of COVID-19 Medications
Antibody therapy and plasma therapy are two non-antiviral tools that HCPs relied upon during the worst waves of the pandemic. Once COVID-19 medications hit the market, they became the go-to treatment for active infections because they successfully interrupt the viral life cycle. But if you find yourself infected with COVID-19, the medication that suits your needs might depend on factors like your age and risk of hospitalization. Each of these drugs works most effectively when taken shortly after the onset of symptoms. Why does when you take the medicine matter? It’s ideal to intervene during the initial stages of infection, before the virus has extra time to damage the body. This is especially important in severe cases, when such damage could be extensive.
As is the case with other viral infections, prioritizing rest and fluid intake can go a long way in COVID-19 recovery. In more severe cases, supplemental oxygen and around-the-clock care might be necessary to help hospitalized patients heal. Without innovative antivirals around yet, early waves of the pandemic relied heavily on supportive care techniques like these. Now approved by regulatory authorities, drugs like nirmatrelvir/ritonavir are quite accessible, as long as you have an HCP’s prescription. They’ve even surpassed supportive treatments and taken center stage as the first line of defense against an active COVID-19 infection due to their efficacy and reliability. Nonetheless, HCPs can use all of these treatment types in tandem to make their combined impact more effective.
Despite all of their advantages, antiviral drugs don’t replace other infection control tactics. Patients using COVID-19 medications are still advised to self-isolate until their infection resolves or, if that’s not an option, wear a mask and practice social distancing. Here, let’s also note that these medications only treat existing cases; they don’t do anything to protect patients against future COVID-19 infection. Instead, those prevention measures are best addressed using vaccines and prophylaxis, two tactics we’ll explore later in this mini-series, as well as old school strategies like good hand hygiene. The classics never go out of style!
Conclusion
The worst of the COVID-19 pandemic has now passed, but epidemiology demonstrates the constant skirmish between the scientific tools underlying public health and the increasing fortitude of formidable pathogens. As we anticipate future pandemics, we can plan ahead by reflecting on our past successes and shortfalls, and now we have effective treatments in case new COVID-19 cases recur in the future. These treatments, though challenging to invent and deploy, represent a great achievement in the biomedical research realm. Although we can’t fully cure viral infections, the good news is that we can prevent them. In a forthcoming article in this public health mini-series, we’ll explore the advanced array of preventive measures — including the groundbreaking mRNA vaccine technology — that stopped COVID-19’s spread in its tracks.
What happens in the body between the time patients are prescribed COVID-19 medications and the time they start to feel better?